FH still remains greatly underdiagnosed, so it is crucial to know whom to screen and to identify index
cases.
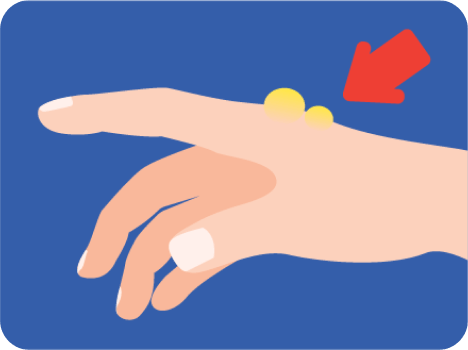
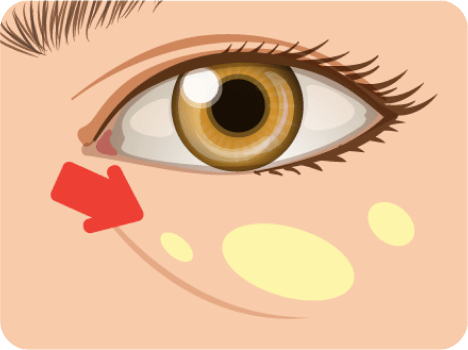
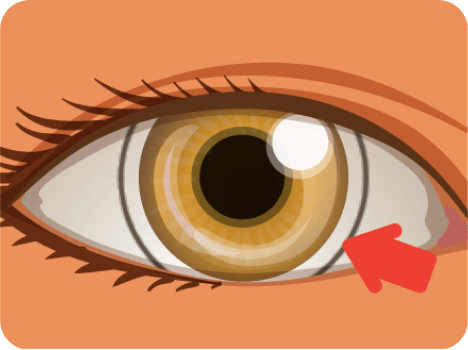
FH should be suspected in individuals with the following findings.1
Establishing the diagnosis should be done as soon as possible for individuals suspected with FH.
Currently, there are multiple diagnostic criteria scores available for FH. They use various FH-related
features to establish the diagnosis (e.g., LDL-C levels, history of CAD, physical examination findings,
family history).1
One of the most commonly used diagnostic criteria is the Dutch Lipid Clinic Network (DLCN). The European Atherosclerosis Society (EAS) recommends to use DLCN for diagnosing FH.2
Dutch Lipid Clinic Network (DLCN)2
EAS Criteria for the Diagnosis of HoFH3
The DLCN score is a validated set of criteria based on
The use of diagnostic tools that rely on the presence of physical features, premature CAD, and
family history limits diagnostic efficacy and the goal of identifying all patients with FH
because although these tools have higher specificity, they have lower sensitivity. Diagnostic
accuracy is key; however, to best identify and subsequently treat the spectrum of patients with
FH (inclusive of those with an identifiable pathogenic variant or variants [genotype positive],
those without [phenotype positive, genotype negative], and those who do not undergo genetic
testing), both genotype-positive and phenotype-positive definitions of FH should be used
Because the FH disease severity varies widely between different genes and within each gene, genetic
testing is a complementary tool for diagnosing FH because it may determine treatment strategies and
the need for screening of family members.4-6
Clinical only
Patient: treat LDL-C
Family: monitor LDL-C and consider treatment
Clinical and genetic
Patient: treat LDL-C
Family: mutation test, monitor LDL-C and consider treatment
Genetic only
Patient: treat LDL-C and consider treatment
Family: monitor LDL-C and consider treatment
The following clinical criteria should be met before genetic testing7
Criteria
Adults
LDL-C > 190 mg/dL
LDL-C > 190 mg/dL
With a known family history of FH
With a parent with FH
With a known family mutation
With parents deceased or unknown
With a family history equivocal or only suggestive of FH
With xanthoma or other physical findings of HoFH or at risk of
HoFHa
With a family history of high cholesterol levels (total, non-HDL-C
and LDL-C) consistent with FH
Based on age- and gender-specific LDL-C
levelsb
With a clinical diagnosis of FH
With suspected HeFHc
With diagnosis of xanthoma or CHD in the family history
With suspected HoFHd
Children
FOOTNOTES
a - By 2 years of age
b - Ideally before puberty
c - Between the ages of 5 and 10
d - Earlier than 5 years of age
Cascade Screening
Cascade screening for FH is an evidence-based intervention that can reduce the
burden of morbidity and mortality from ASCVD and has been recommended by
national and international organizations2,8
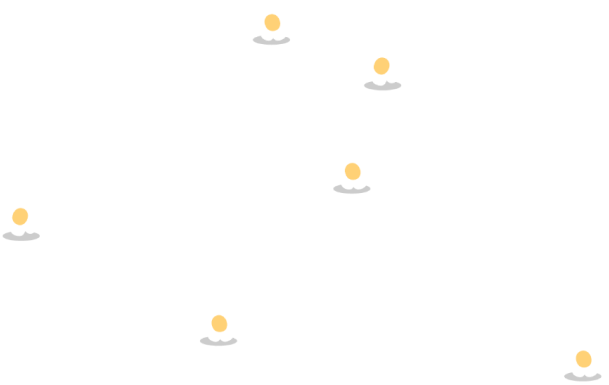
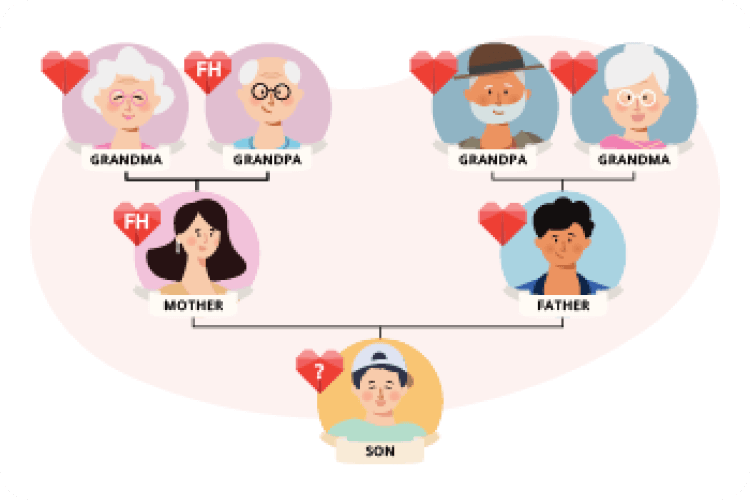
Cascade screening is an active process to screen and test the relatives of the patients’ with genetic conditions that may “run in the family”.
As FH is dominantly inherited, cascade screening of family members can be highly effective to know whether any individuals in the family have FH.
Once a FH patient (index case) is identified, several cycles of cascade screening are required to identify all patients with FH in their family. Screening cycles are repeated (cascaded) for each relative diagnosed with FH, thereby expanding the number of potential cases detected.
Cascade screening8
Reverse cascade screening 9,10
Screen cycle 1
Once an index patient with FH is identified, cascade screening starts with first-degree relatives (parents, siblings, children)
Screen cycle 2
If the affected parent is identified, as many relatives as possible on that parent’s side of the family should be screened
Screen cycle 3
Children of the affected parent’s siblings should also be screened because treatment in childhood is indicated for those who are affected
Screen cycle 4
Each new FH case found via cascade screening then becomes an “index case” for broader cascading
Reverse cascade screening (or child-parent screening)
can be used to identify most families with FH in a population.
The process means:
Children are tested for the
LDL-C levels in routine immunizations
(normally at age 1–2 years)
If a child tests 'positive'
(> 1.5 times the median LDL-C levels of age-specific population) the parents will be tested
There is a 96% chance
that is an affected parent will be correctly identified.
REFERENCES:
Ison HE, et al. Familial Hypercholesterolemia. 2014 Jan 2 [Updated 2022 Jul 7]. In: GeneReviews®. Seattle (WA): University of Washington, Seattle. Available from: https://www.ncbi.nlm.nih.gov/books/NBK174884/
Nordestgaard BG et al. Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: guidance for clinicians to prevent coronary heart disease: consensus statement of the European Atherosclerosis Society. Eur Heart J. 2013; 34:3478a-3490a.
Cuchel M, et al. 2023 Update on European Atherosclerosis Society Consensus Statement on Homozygous Familial Hypercholesterolaemia: new treatments and clinical guidance. Eur Heart J. 2023;44(25):2277-9
National Institute for Health and Care Excellence. Familial hypercholesterolaemia: identification and management. Appendix F: Simon Broome criteria. 2008. Available at https://www.nice.org.uk/guidance/cg71/evidence/full-guideline-appendix-f-pdf-241917811. Accessed on 16 Nov 2022.
De Castro-Orós I, et al. The genetic basis of familial hypercholesterolemia: inheritance, linkage, and mutations. Appl Clin Genet. 2010;3:53-64.
Foody JM, et al. Familial hypercholesterolemia/autosomal dominant hypercholesterolemia: Molecular defects, the LDL-C continuum, and gradients of phenotypic severity. J Clin Lipidol. 2016;10:970-986.
Migliara G, et al. Familial Hypercholesterolemia: A Systematic Review of Guidelines on Genetic Testing and Patient Management. Front Public Health. 2017;5:252.
Knowles JW, et al. Cascade Screening for Familial Hypercholesterolemia and the Use of Genetic Testing. JAMA. 2017;318(4):381-382.
Morris JK, et al. The evaluation of cascade testing for familial hypercholesterolemia. Am J Med Genet A. 2012;158A(1):78-84.
Wald DS, et al. Child-parent screening for familial hypercholesterolaemia: screening strategy based on a meta-analysis. BMJ. 2007;335(7620):599.
Sturm AC, et al. Clinical Genetic Testing for Familial Hypercholesterolemia: JACC Scientific Expert Panel. J Am Coll Cardiol. 2018;72(6):662-680